|
DENTAL AMALGAM
a. History of Amalgam. Dr. G. V. Black investigated the properties of amalgams and their possible use for dentistry about 1895. His studies showed the effects of chemical composition and physical structure on the properties of amalgam restorations. Due largely to the work done by Dr. Black and the National Bureau of Standards, and other researchers, amalgam is now used more than any other filling material for the restoration of posterior teeth.
b. Definitions.
(1) Alloy. An alloy is a solid mixture of two or more metals. It is possible to produce a material in which the desirable properties of each constituent are retained or even enhanced, while the less desirable properties are reduced or eliminated. With few exceptions, the metals used in dentistry are in fact alloys.
(2) Amalgam. When one of the metals in an alloy mixture is mercury, an amalgam is formed. A dental amalgam is a combination of mercury with a specially prepared silver alloy, which is used as a restorative material.
(3) Mercury. Mercury is a silver-white, poisonous, metallic element that is liquid at room temperature (symbol Hg).
c. Composition and Effects of Amalgam.
(1) Combining desirable properties. Each metal incorporated into a dental silver alloy has specific properties when combined with mercury. Some properties are desirable and some are undesirable. An acceptable alloy is balanced. The combined effects of the properties of its ingredients should provide the most satisfactory restorative material.
(2) Quantity of mercury. Too little mercury in the mix results in a grainy, weak, readily tarnished, and corroded amalgam. Too much mercury will cause excessive expansion and weakened amalgam.
(3) Standards and requirements. Like other restorative materials, amalgam must meet the standards and requirements set by the National Bureau of Standards and the American Dental Association's (ADA) Specification #1 for alloy used in amalgam.
(4) Composition of the alloy. The ADA specification states that the composition of the alloy must include a minimum of 65 percent silver, a maximum of 29 percent tin, a maximum of 6 to 13 percent copper, and a maximum of two percent zinc by weight. See figure 1-1.
(5) Correct proportion important. Immediately prior to use, the silver alloy is mixed with pure and uncontaminated mercury. (Mercury, although an indispensable ingredient, imparts undesirable properties to the amalgam if added in incorrect proportions.) There are some alloys that are completely zinc free. They can therefore be used more successfully in a moisture-contaminated environment.
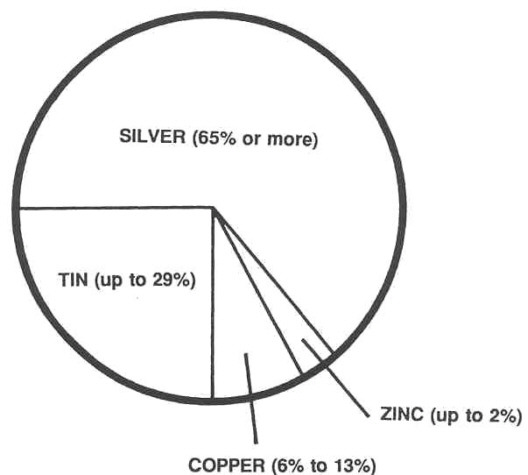
Figure 1-1. Approximate composition of an acceptable amalgam alloy.
(6) Properties of the finished product. Each element composing amalgam imparts certain properties to the finished product. Table 1-1 summarizes these properties. Silver imparts strength, durability, and color, gives the alloy desirable setting expansion, decreases flow, and accelerates (decreases) the setting time. Tin makes the amalgam easier to work, controls excessive setting expansion, and increases both flow and setting time. Copper increases hardness, contributes to setting expansion, reduces flow, and decreases setting time. Zinc increases workability, and unites with oxygen and other "impurities" to produce a clean amalgam.
|
PROPERTY
|
INGREDIENT
|
|
Silver
|
Tin
|
Copper
|
Zinc
|
| Strength |
Increases
|
|
|
|
| Durability |
Increases
|
|
|
|
| Hardness |
|
|
Increases
|
|
| Expansion |
Increases
|
Decreases
|
Increases
|
|
| Flow |
Decreases
|
Increases
|
Decreases
|
|
| Color |
Imparts
|
|
|
|
| Setting time |
Decreases
|
Increases
|
Decreases
|
|
| Workability |
|
Increases
|
|
Increases
|
| Cleanliness |
|
|
|
Increases
|
Table 1-1. Effects on properties of an amalgam restoration imparted by ingredients.
|
d. Physical Properties of Amalgam. The most important physical properties of amalgam are flow and creep, dimensional change, and strength.
(1) Flow and creep. Flow and creep are characteristics that deal with an amalgam undergoing deformation when stressed. The lower the creep value of an amalgam, the better the marginal integrity of the restoration. Alloys with high copper content usually have lower creep values than the conventional silver-tin alloys.
(2) Dimensional change. An amalgam can expand or contract depending upon its usage. Dimensional change can be minimized by proper usage of alloy and mercury.
(3) Compression strength. Sufficient strength to resist fracture is an important requirement for any restorative material. At a 50 percent mercury content, the compression strength is approximately 52,000 pounds per square inch (psi). In comparison, the compressive strength of dentin and enamel is 30,000 psi and 100,000 psi, respectively. The strength of an amalgam is determined primarily by the composition of the alloy, the amount of residual mercury remaining after condensation, and the degree of porosity in the amalgam restoration.
ADVANTAGES AND DISADVANTAGES OF AMALGAM
a. Advantages. Amalgam has many advantages over other materials as a restorative material. Amalgam is used more than any other material to restore carious teeth. It is easy to insert into the cavity preparation and adapts readily to cavity walls. In obtaining its initial set, or hardness, amalgam allows time for condensing and carving. It has an acceptable crushing strength and is recognized as having a long life as a restoration. As an amalgam restoration ages in the oral cavity, corrosion products form along the restoration-tooth interface. These compounds act as a mechanical block to microleakage and account for the excellent clinical results obtained with silver amalgam.
b. Disadvantages. Amalgam has many disadvantages as a restorative material. Because amalgam's color does not match the color of the teeth, it is generally not used on the visible surfaces of anterior teeth. Amalgam will tarnish with time, no matter how well the amalgam restoration is prepared and inserted. To avoid or to reduce tarnish, the restoration is smoothed and highly polished a day or two after its insertion. The restoration may be reshined later at any time with little effort. Amalgam will also conduct heat or cold readily (high thermal conductivity). If the amalgam is placed too close to the pulp, it may irritate the pulp. Therefore, an intermediate base that will not conduct heat or cold as readily (low thermal conductivity) is placed under the amalgam.
USAGE AND PREPARATION OF AMALGAM
a. General. The dental specialist has the direct responsibility for the correct preparation and use of amalgam. Incorrect use may produce a faulty restoration that can cause or contribute to the loss of a tooth. Therefore, the dental specialist must use extreme care in preparing a good mix of amalgam that will provide the best qualities obtainable from the alloy.
b. Proportioning Alloy and Mercury. To proportion and mix dental alloy and mercury, the size of the mix (the number of alloy pellets to be used) and the alloy-mercury ratio must be known. The dental officer determines the size of the mix used. Dental alloy is supplied in pellet form or in sealed capsules containing premeasured mercury. The pellets are composed of silver alloy filings compressed under pressure without a binding agent. They are supplied in weights ranging from 4.8 to 6 grains per pellet. A special dispenser is used to drop the pellets individually. (See figure 1-2.) Since the pellets are preformed in a set amount of silver alloy, only the amount of mercury used with each pellet needs to be measured. The mercury dispenser is furnished with four interchangeable plungers lettered A through D. (See figure 1-2.) The manufacturer's instructions accompanying the pellets should be followed in selecting the size of plunger to use in providing the desired ratio of alloy to mercury. The alloy-mercury capsules are preweighed and premeasured, needing only to be combined internally. This is done by penetrating a membrane separating the alloy and mercury prior to trituration.
c. Trituration of Amalgam. Trituration is the mechanical mixing of the alloy and mercury. Trituration is done by hand using a mortar and pestle or a mechanical amalgamator. (See figure 1-3.) Trituration is done by setting the timer according to the manufacturer's instructions for the alloy and for the type amalgamator used. Special capsules are furnished with the mechanical amalgamator to hold the alloy-mercury mixture during trituration. Each capsule is fitted with a cap and a small rod-like pestle. A small funnel is also furnished to help in pouring the mercury into the capsule. The
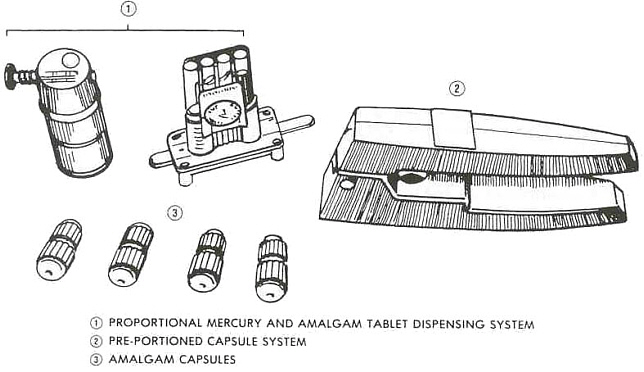
Figure 1-2. Amalgam dispensing systems.
amalgamator mixes the amalgam in the capsule by rapid shaking or vibration. This produces a consistently uniform mix. The amalgamator reduces trituration to a matter of seconds. When using the pellet method, first insert the pestle in the capsule, dispense the required mercury, and then dispense the pellets. Usually one pellet is used for a small mix and two pellets for a large mix. Most manufacturers recommend mixing times of approximately 10 seconds per pellet. When the time selected has elapsed, the automatic timer will stop the machine. The dental specialist must be careful not to overtriturate or undertriturate. Overtrituration results in shorter setting time and increased shrinkage. Undertrituration results in increased expansion, lengthened setting time, and weakened amalgam.
d. Filling Amalgam Carrier. Modern dental amalgams use precise proportioning methods for dispensing the mercury with the alloy. Since the mercury content in the original mix is less than the maximum level of 55 percent, it is not necessary to eliminate mercury from the amalgam before it is carried to the cavity preparation. The amalgam is taken from the capsule and placed in an amalgam cup. The amalgam carrier is loaded by forcing the open cylinder of the amalgam carrier into the balled amalgam. The amalgam is then carried to the mouth and deposited in the cavity preparation.
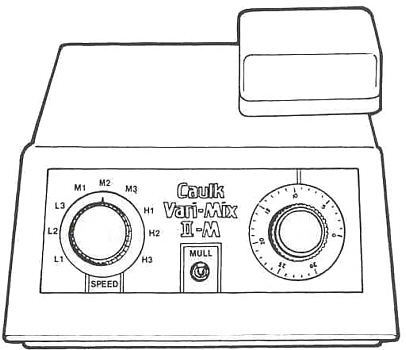
Figure 1-3. Mechanical amalgamator.
e. Condensation and Carving of Amalgam. Condensation is the process of packing an amalgam mix into a cavity preparation. Both time and pressure are important to achieve the best results. Condensation must be accomplished before crystals start to form. Delay will result in a breakdown of these crystals and a weakened amalgam. Sufficient condensation pressure is necessary to prevent voids in the restoration. The amount of pressure varies with each type of amalgam. Usually the amalgam restoration is well set and hardened so that carving can be started with sharp instruments immediately after condensation. The carving operation results in a completely restored tooth.
PRECAUTIONS DURING AMALGAM PREPARATION
a. Moisture Contamination.
(1) Four possible adverse effects.
(a) Excessive expansion of the amalgam.
(b) Postoperative pain.
(c) Lowered crushing strength.
(d) Blister formation on the surface of the amalgam.
(2) Avoidance procedures. Moisture can be introduced into amalgam by triturating below the dew point (temperature at which moisture collects on a surface). Moisture can also be introduced by the presence of moisture in the cavity being filled or by accidental contact with saliva. To avoid moisture contamination, all instruments and equipment encountering the amalgam should be dry. The temperature of equipment and materials should be high enough so that no moisture collects. Saliva should be kept out of the cavity preparation during the insertion of the material.
b. Guidance for Amalgam Preparation. Any portion of amalgam that is too dry or has begun to crystallize must be discarded. Its use would result in a weak, nonhomogeneous mass. For large restorations, it may be necessary to prepare two or more mixes. Each mix is prepared as needed.
c. Training of Personnel Required. All dental personnel must be familiar with the potential hazards and the proper handling of mercury.
MERCURY HYGIENE PRACTICES BY THE DENTAL SPECIALIST
a. General. Amalgam restorations do not constitute a hazard to patients. However, dental personnel may invite a health hazard if exposed to concentrated mercurial vapors over an extended period of time. Mercury hygiene precautions should be used.
b. Mercury Hygiene Precautions.
(1) Training. All dental personnel must be instructed regarding the potential health hazards of mercury and what constitutes proper handling.
(2) Covering cuts and abrasions. All cuts and abrasions of the skin must be covered when handling amalgam or mercury.
(3) Washing hands and arms. All dental personnel must wash hands and arms thoroughly after amalgam operations.
(4) Inspection of capsules. Capsules must be checked for general condition and seal. Cracked capsules or those in poor condition will be discarded.
(5) Use of masks. All dental personnel must wear masks when removing amalgam restorations.
(6) Use of water coolant. A water coolant must be used to reduce and minimize the dispersion of particles during removal of amalgam restorations.
(7) Use of gloves. Handling amalgam with bare hands must be avoided.
(8) Use of standard containers. An amalgam well or a dappen dish must be used to hold prepared amalgam.
(9) Storage of materials. Old amalgam and mercury must be stored under fresh, clean fixer solution in strong, closed containers in a cool, fireproof area.
(10) Disposal of wastes. Disposable paper, cloths, and rubber items that are mercury or amalgam contaminated must be deposited into bag-lined, covered containers after use. Bag and contents must be disposed of daily.
(11) Avoiding heat. Amalgam mixing equipment, as well as mercury, must be kept away from any source of heat.
(12) Use of closed containers for amalgamators. Amalgamators must be kept inside closed containers as much as possible.
(13) Weekly cleaning of amalgamators. Amalgamators must be cleaned at least once a week.
(14) No carpeting in work area. There must be no carpeting in the part of the dental clinics where mercury or amalgam are used.
(15) Separate area for cleaning. The cleaning area for equipment for laboratories and other clinic areas must be kept separate and distinct from the cleaning area for equipment used with amalgam or mercury in order to avoid wide dispersal of mercurial vapors.
|