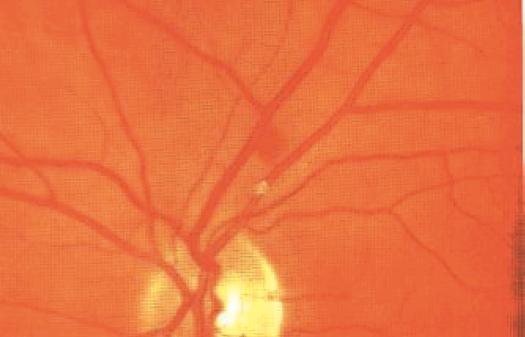
Cholesterol embolus in the fundus الصمة الكوليسرولية في قعر العين
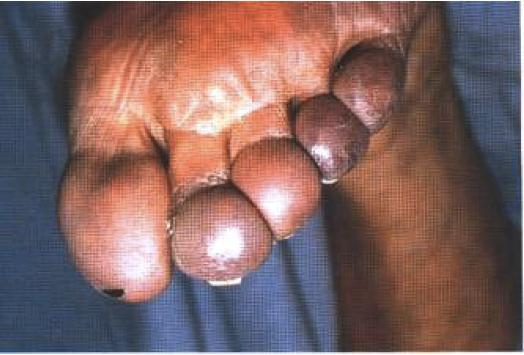
INSTRUCTION Examine this patient's fundus. SALIENT FEATURES History * Severe, acute and painless diminution or loss of vision. · History of atherosclerosis. · Risk factors of atherosclerosis: family history, diabetes, hypertension, ischaemic heart disease, peripheral vascular disease, cerebrovascular disease. Examination Presence of a cholesterol embolus (Hollenhorst plaque; Fig. 83) in one of the branches of the retinal artery. Proceed as follows: · Look for a cherry-red spot at the fovea (the ischaemic retina at the posterior pole becomes milky white and swollen, and the choroid is seen through the fovea as a cherry-red spot). · Tell the examiner that you would like to check for visual field defects. Remember that retinal artery occlusion results in infarction of the inner two thirds of the retina, reflex vasoconstriction of the retinal arterial tree and stasis in the retinal capillaries. DIAGNOSIS This patient has a cholesterol embolus in one of the branches of the retinal artery (lesion) due to underlying atherosclerotic disease (aetiology). Read classic review on this subject: N Engl J Med 1993; 329: 427. QUESTIONS What are the complications of such an embolus? Retinal artery occlusion causing field defects or loss of vision. Where is the likely origin of this embolus? The most likely origin is an atherosclerotic plaque in the carotid circulation. What are the causes of retinal arterial occlusion? The commonest cause is emboli arising from the major arteries supplying the head or /'rom the left side of the heart. Embolic particles consist of platelet clumps, cholesterol crystals or Hollenhorst plaques and others (mixed thrombus, calcific or septic material from cardiac valves, fat, myxoma, talc in intravenous drug abusers or silicone in those who receive injections for cosmetic purposes). Other causes include: · Temporal arteritis. · Collagen vascular diseases. · Increased orbital pressure, e.g. retrobulbar haemorrhage, Graves' exophthalmos. · Sickle cell disease. · Acute arteriolar spasm due to intranasal cocaine. · Syphilis. What do you understand by the term 'amaurosis'? Amaurosis means blindness from any cause. What do you understand by the term 'amblyopia'? Amblyopia means that impaired vision is not due to refractive error or ocular disease. What do you understand by the term 'amaurosis fugax'? Amaurosis fugax is a retinal artery transient ischaemic attack (TIA) which mani-fests with a painless, unilateral loss of vision that usually lasts a few minutes. How would you manage this patient? · Aspirin. · Ophthalmology opinion. · Ultrasonography of the carotid arteries. · Advise the patient to stop smoking. · Control of hypertension. · Carotid angiography with a view to performing carotid endarterectomy. What is the effect of cholesterol crystals? Cholesterol crystals rarly cause significant obstruction to the retinal arterioles. What manoeuvre would you use to make the cholesterol crystals more apparent? Mild lateral pressure on the globe may make the presence of unobtrusive crystals clearly visible when the retinal arteries pulsate. How would you manage an acute occlusion of the retinal artery? · Lie the patient in a supine position to ensure adequate circulation. · Apply intermittent ocular massage for 15 minutes to dislodge the emboli, lower intraocular pressure and improve circulation. · Intravenous acetazolamide to lower intraocular pressure. · Inhalation of a mixture of 5% carbon dioxide and 95% oxygen. · Anterior chamber paracentesis. If the investigation of a patient with amaurosis fugax provides no evidence of carotid artery disease, embolism or other recognized causes of the disorder, then the diag-nosis by exclusion should be vasospasm. In such cases a calcium channel blocker should be tried. What do you know about the 'purple toe syndrome'? This was first described with warfarin therapy by Feder and Auerbach in 1961 and was shown to be caused by showers of atheroemboli (Ann Intern Med 1961: 55: 911-17). Now, with the increasing use of coronary angioplasty and thrombolytic therapy in the elderly, cholesterol emboli are increasingly reported. They result in 'purple toes' (Fig. 84), amaurosis fugax, and atheroembolic disease of kidneys, skin and gastrointestinal tract.